A vaccine consent form is quite important when it comes to the vaccination process at a healthcare organisation. Here you can find the vaccine consent form template that you can download and use directly.
All licensed medical practitioners use a vaccine consent form to remain protected against unfair lawsuits. In order to read more about vaccine consent form and when it is crucial to use it, keep reading the information below:
What Is a Flu Shot Vaccine Consent Form?
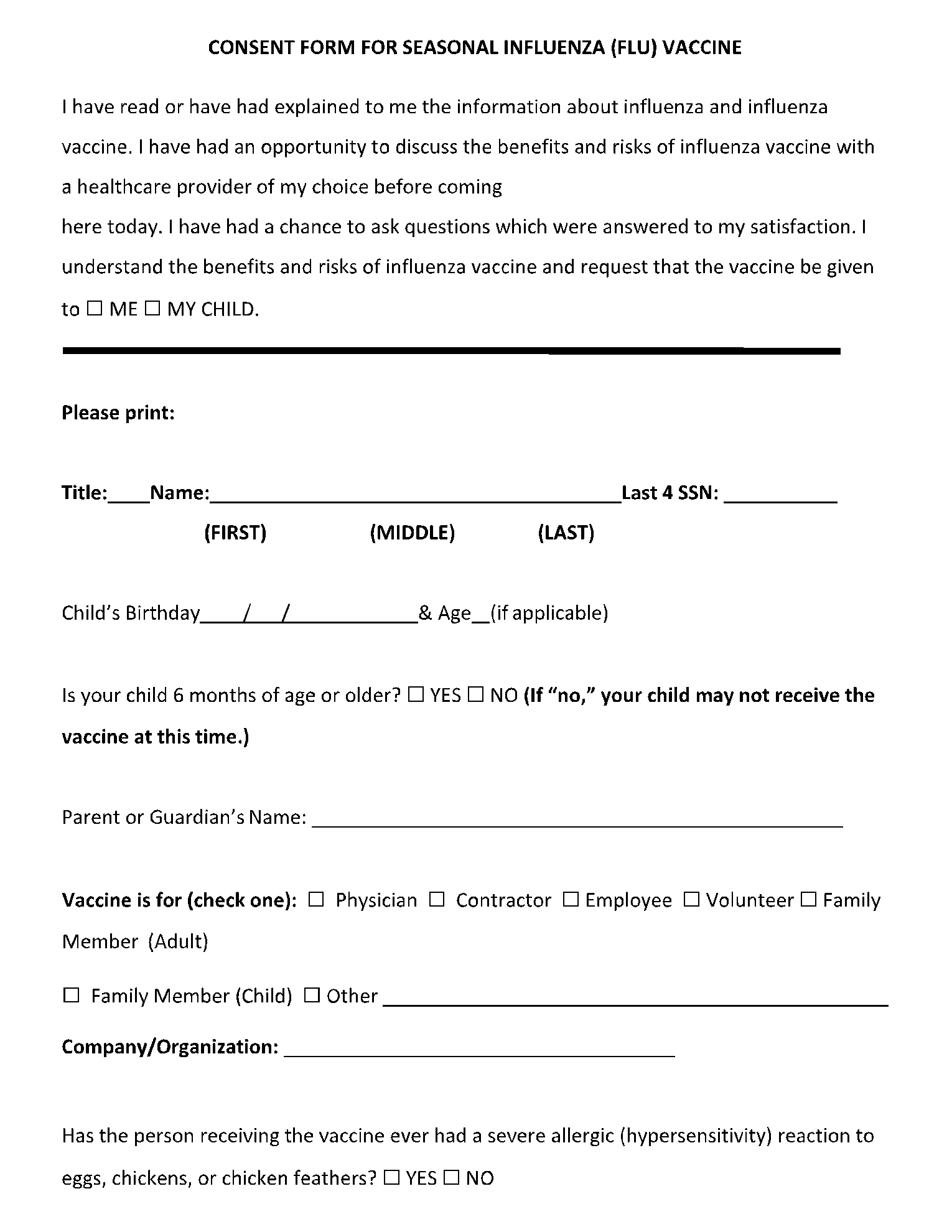
A flu shot vaccine consent form gives a nurse or a doctor the permission to go ahead and administer the patient with the flu vaccine.
This form is signed by the person who is going to be vaccinated. In case the person to be vaccinated is a minor, the consent form should be signed by the parents or the guardian.
What Are Included in a Flu Shot Vaccine Consent Form?
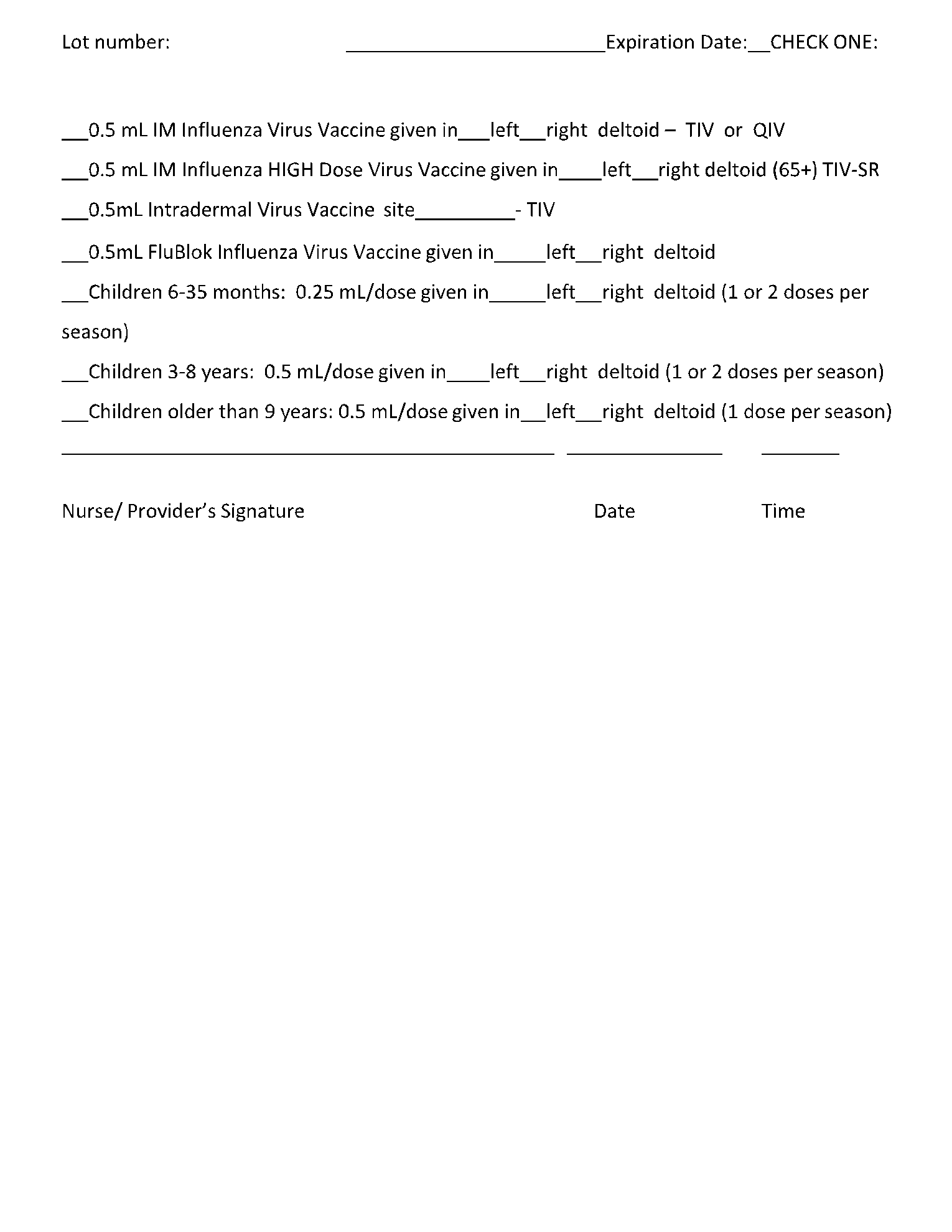
The flu shot vaccine consent form contains the full name of the person who is to be vaccinated, along with the details of the healthcare administrator.
Through the form, the person consents to the fact that they are agreeing to the flu shot vaccine and they understand the possible side effects of the same.
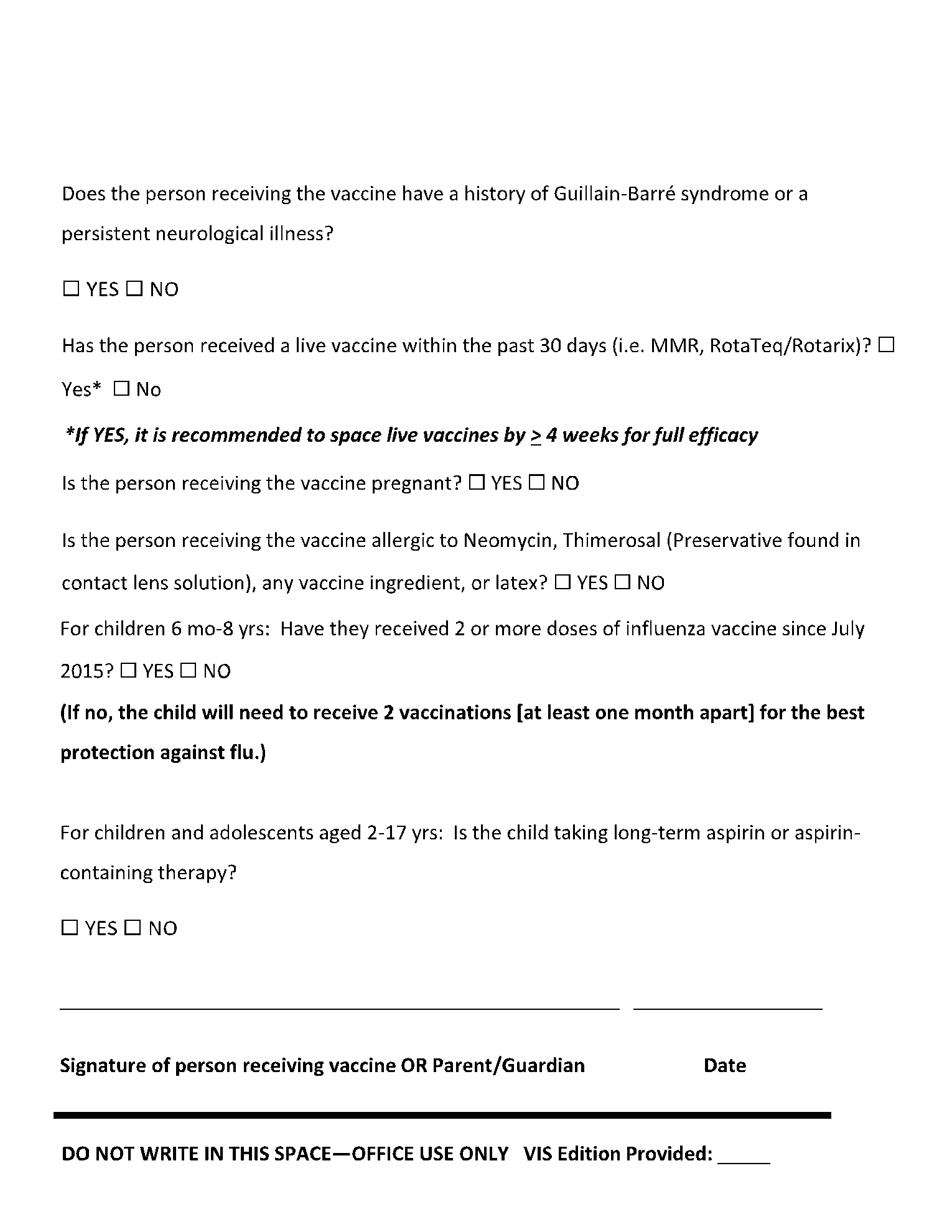
The flu shot vaccine consent form also contains some questions to make sure that any person who might be at risk from the vaccine can avoid it, and it protects the healthcare administrator from any unforeseeable accidents that are not caused by intention.
It is best to use the flu shot vaccine consent form along with a detailed conversation with the person to explain to them the possible allergic reactions to the vaccine.
Endnotes
Vaccine consent forms are very important to protect medical practitioners from any lawsuits that aren’t because of their fault. In order to create a vaccine consent form, all that is needed is to download the vaccine consent form template from CocoSign.
CocoSign offers various form templates ready to download with a single click. These templates can also be edited to include any additional requirements that you might have.