A power of attorney is a legal document where you can appoint and authorize a trusted person to make decisions for you under different circumstances.
There are different types of power of attorney, such as durable and non-durable, springing, financial, and medical. The basic principle of all these types of POAs are the same – they enable another trusted person known as an ‘agent’ to make decisions on your behalf.
But each of these POAs is different in some aspects such as what decisions you allow the agent to make and when and how the document comes into effect.
In this post, we’ll explain in detail the Texas medical power of attorney, such as what it is and how it works.
What is a Texas Medical Power of Attorney?
The medical power of attorney Texas is used to grant authority to an agent to make healthcare decisions for you when you are incapable of making the decisions yourself.
Healthcare decisions involve things such as choosing the proper course of treatment for your condition, accepting or denying certain treatment methods or medications, accessing your medical history, and even something as serious as choosing to end life-support.
The person that authorizes the agent to make decisions for him/her is called the ‘principal.’ By signing the medical power of attorney as a principal, you are essentially allowing the agent to make crucial decisions regarding your health and medical treatment that might even involve life and death situations.
That is why you must be extremely careful and selective about choosing the most trustworthy person – be it a family member, relative, or a close friend – as the agent.
Why and When Do You Need a Texas Medical Power of Attorney?
Generally speaking, you should have a medical power of attorney form Texas in place if you are suffering from a condition that is severe and will most likely leave you incapacitated or unable to make decisions for yourself in the future.
One of the most common use cases of medical power of attorney is for senior citizens and older people unable to look after their own health effectively in Texas.
But even if you’re young and not suffering from any severe medical conditions, you are still free to get a medical power of attorney in place to prepare for unforeseen health issues in the future. Yet it’s mainly old and aging people, disabled people, and those suffering from long-term medical conditions that need a Texas medical power of attorney.
What is the Importance of Medical Power of Attorney?
If sudden complications in your health leave you in a difficult state, such as incapacitated or in a coma, then it becomes very difficult and complicated to determine who should have a say in your treatment. Or, if you’re a senior citizen with deteriorating mental and cognitive skills, you might not be able to make the best healthcare decisions for your good.
In such cases, it’s important to have a trusted person, one that cares for your well-being as an agent. And as already mentioned before, there can be life and death situations due to health complications.
Without an agent to act on your behalf, precious time will be wasted in determining who should make decisions in such situations. Hence, the medical power of attorney can be extremely useful in crucial, time-sensitive medical conditions.
What Does a Texas Medical Power of Attorney Include?
The Texas Medical Power of Attorney allows your agent to make any decisions related to your healthcare and medical treatment. But there are some decisions that the agent cannot make such as:
- Consent to neurosurgery and abortion
- Denying treatment that is sure and certain to improve your health condition or provide temporary comfort
Also, keep in mind that your agent cannot be your doctor or the primary health care professional looking after your condition, nor can it be any other person employed by them.
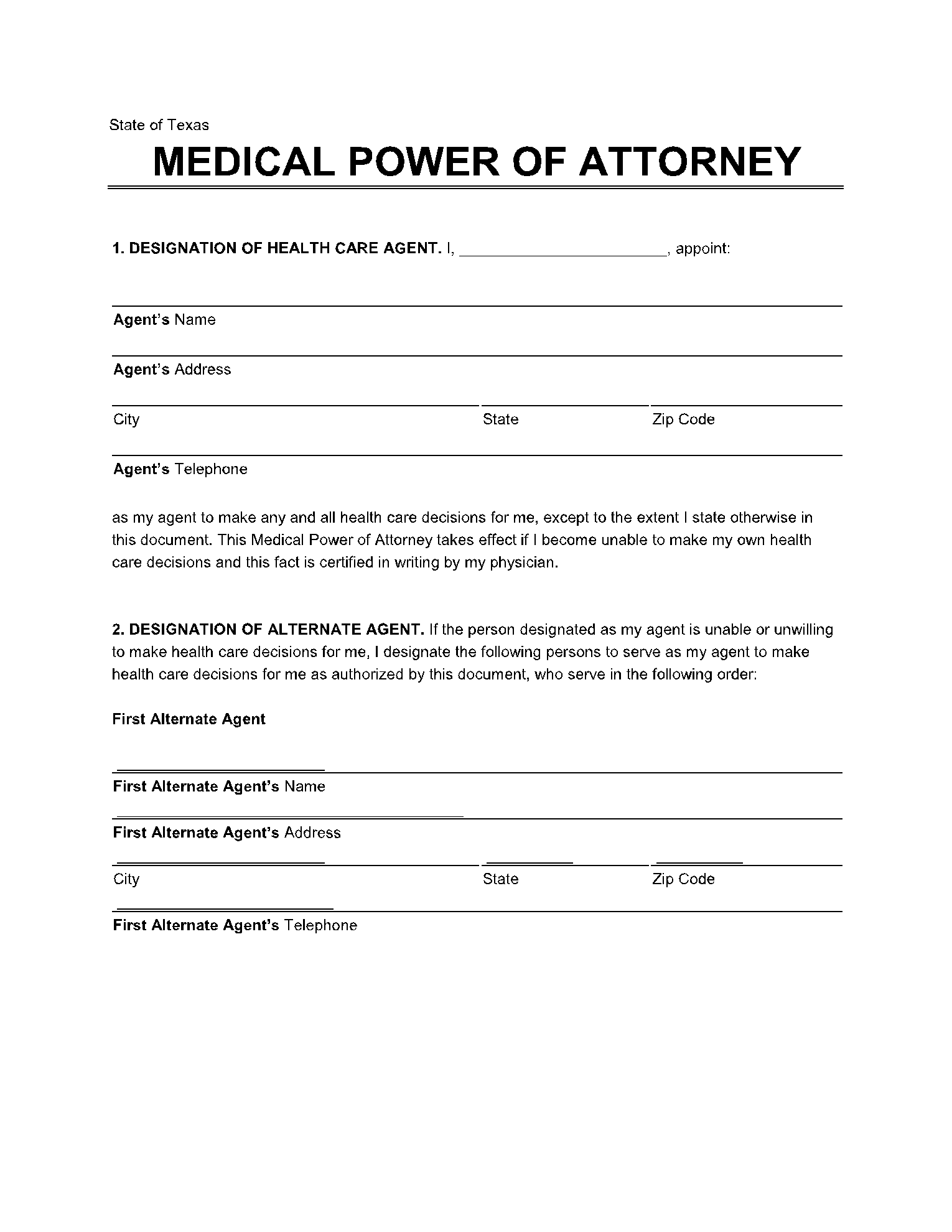
The Texas medical power of attorney form requires the following details:
- The names of both principal and agent, along with their addresses and contact number.
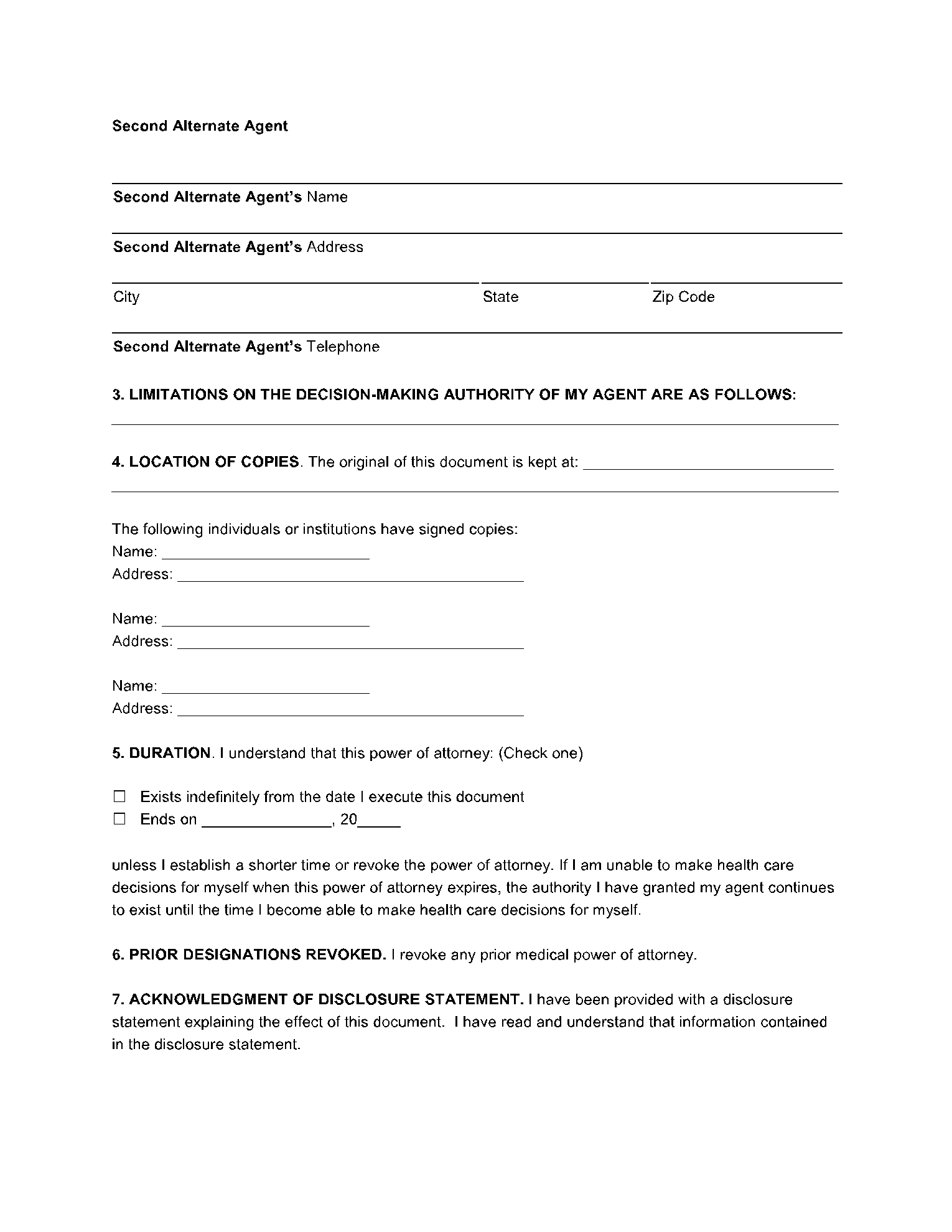
- A box to specify if the principal wants to place any limitations on the decision-making authority of the agent.
- Name and details of two alternate agents (in case the main agent is also rendered incapable of making decisions somehow). However, this field is not mandatory.
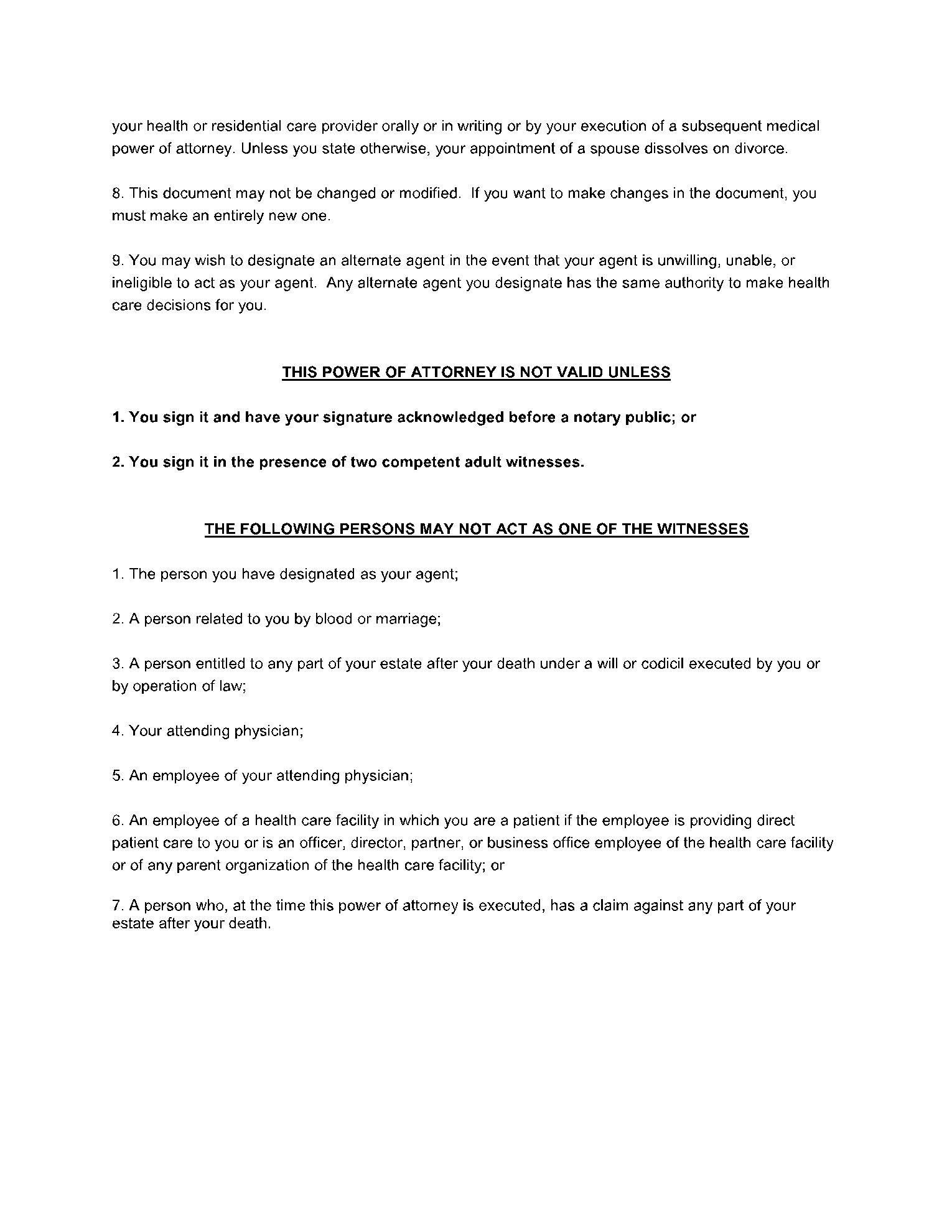
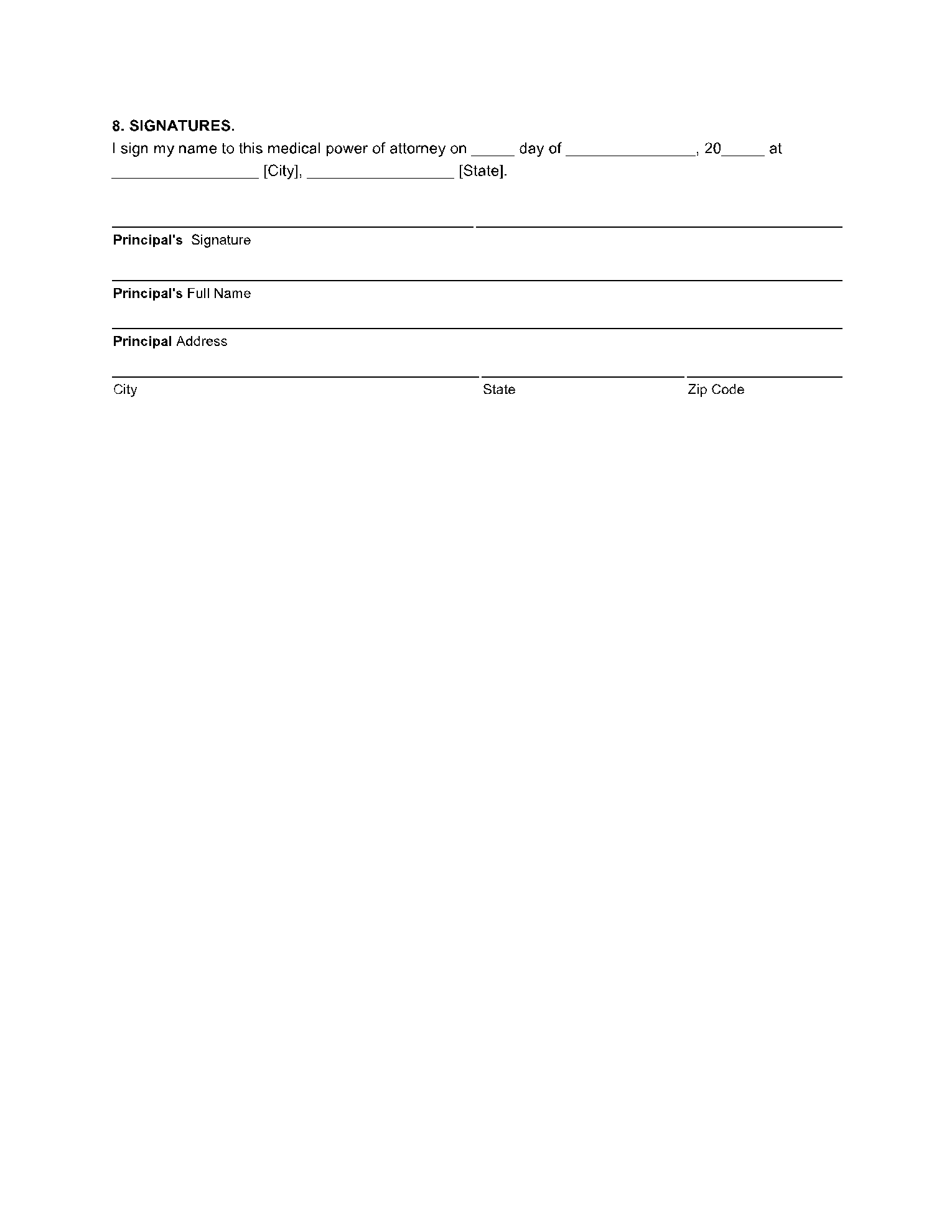
- Statement and signature of two witnesses OR the signature from a notary
Other Key Factors You Should Know About Texas Medical Power of Attorney
Here are some minor, yet essential details about the medical power of attorney Texas form:
- You can decide if a power of attorney comes into effect immediately after obtaining all signatures or in the future, only after you become incapable of making your own decisions.
- You can set an expiration date for your power of attorney, after which it gets automatically revoked.
- If you choose to get signatures of two witnesses, they must both be adults. One out of the two witnesses must be someone that is not: the agents themselves; your doctor/medical care providers or their employees; your spouse or relative; any person who has some claim over your will or estate.
The Texas Medical Power of Attorney is essential if you are aging or suffering from a serious illness. But we do recommend that you choose your agent with extreme care and put a lot of thoughts into it. If you have decided to set up a medical power of attorney, you can easily download the required templates from CocoSign, where you’ll find hundreds of templates for all types of power of attorney forms.